What are the EMFIS diagnostic criteria?
How can EMFIS be diagnosed, i.e. on which diagnostic criteria can this new pathology be recognized? In the presence of a patient claiming to be EHS, the physician should first listen to him carefully, with an open, curious mind, trying not to systematically question the declarations, even if they appear at first glance unrealistic. The main clinical goal is an attempt at recovering the facts, especially at the time of their occurrence. The physician must take into account that patients often have cognitive impairment as a result of EMFs exposure, including possible abnormal behaviors as emotion, nervousness, irritability. Trying to understand the patient and his disease is the priority. The physician must therefore not exclude EMFs before a thorough and precise interview and a rigorous and comprehensive physical and neurological examination; performing usual biologic and imaging tests (cerebral scan or MRI, carotid ultrasound Doppler and angiography if necessary) to exclude any known organic pathology.
Physicians should not be misled by the usual normality of these investigations. Because the normality of classical brain imaging investigations can actually be a major positive diagnostic sign of EMFIS, at least before the occurrence of complications.
The following diagnostic arguments will be retained for EMFIS:
1 Clinically

- The chronological sequence of functional symptoms, i.e. their appearance and disappearance depending on electromagnetic sources exposure. This research is sometimes difficult, hence the need for a careful and comprehensive interview.
- The complete exposure history to electromagnetic sources (several hours a day for several years), whether radio or high frequencies (mobile phone, cordless phone, geo-localization device, usage habits, etc ....), or low or extremely low frequencies (high or very high voltage power lines, electric transformers, house appliances etc. ...).
- The progressive completeness of the clinical features through collecting functional symptoms and identification of physical signs (erythema, joint damage, Romberg sign, etc. ... ).
4 The normality of usual medical imaging investigations (brain scan and / or MRI, carotid Doppler).
5 The past or current existence of dental alloys or metal prostheses acting as "antenna" and thus promoting EHS and consequently the occurrence of clinical symptoms.
6 The existence of a family history of EHS and / or of Alzheimer's disease.
7 The existence of an intolerance to chemicals or the association with a true evolved MCS.
8 Above all the absence of any other disease or pathological disorder that could account for the observed symptoms: classical migraine, ear infections, degenerative neuropathy, viral hepatitis, cancer, dermatitis, arthritis, osteoarthritis, psychiatric illness, etc. ...).
Thus, as a first step, it is essentially a diagnosis of exclusion that is proposed before considering in a second step the positive biological diagnosis of the disease.
2. Biologically
The diagnosis relies on the four following objective elements:
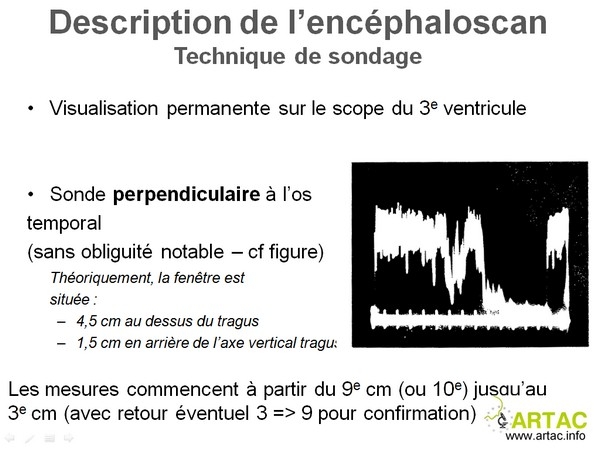
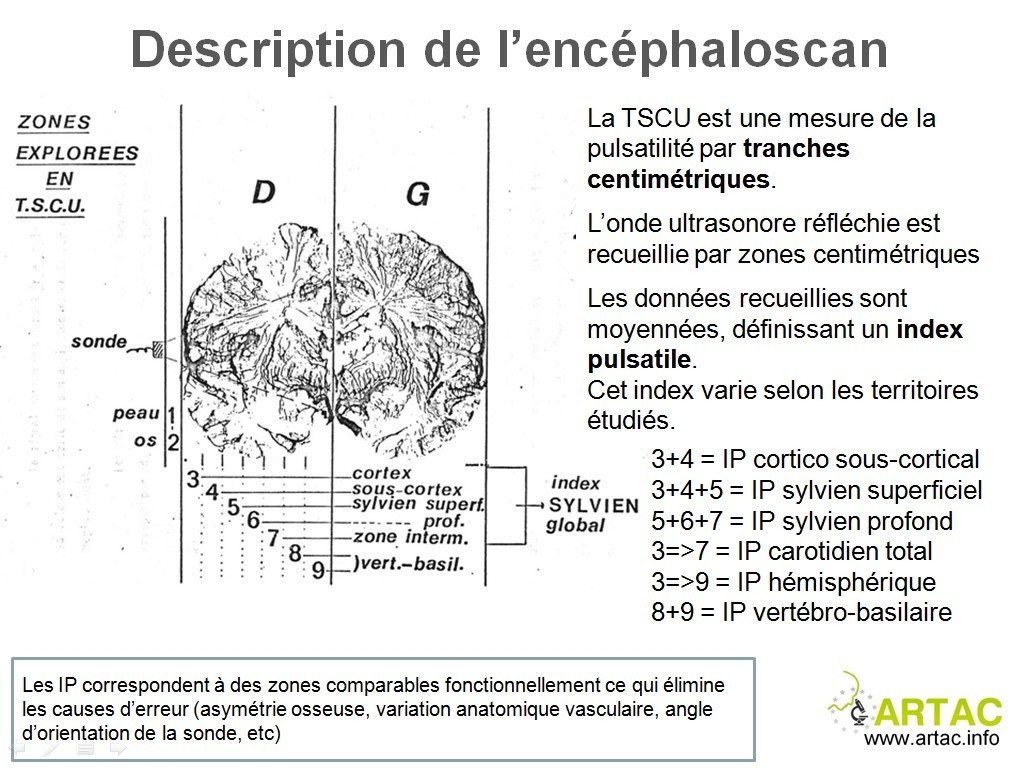
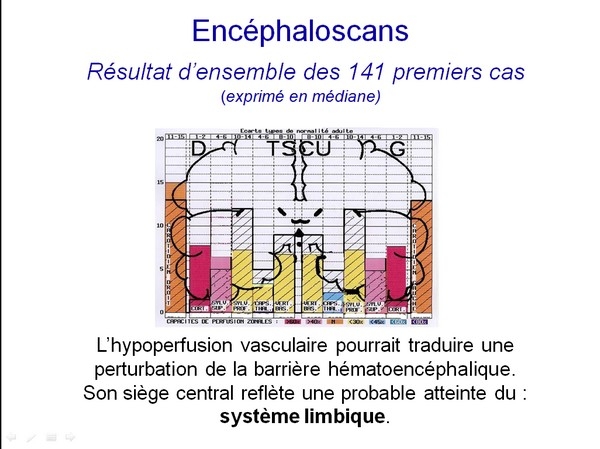
1 . The evidence of a cerebral hypo-perfusion by measuring the blood flow velocity in the middle cerebral artery by cerebral echo-Doppler, with confirmation by pulsed cerebral echo Doppler (encephalo-scan) focused on the temporal lobes that the decrease in cerebral blood flow, concerns in particular the areas corresponding to the limbic system and / or to the thalamus.


2 . The evidence of biologic abnormalities such as previously individualized. In the blood: an increase in histamine and S100B protein, the presence of anti O-myelin, anti- Hsp27 and Hsp70 antibodies; a decrease in vitamin D; an increase in nitrotyrosamine suggesting a decrease in the anti-oxidant defenses. In 24-hour urine: either a decrease or an increase in melatonin excretion.
3 . In difficult cases, the performing of a provocation test using standardized conditions.
4 . In all the cases, the use of treatment as a therapeutic test and the use of preventive measures as electromagnetic weaning test.
Using such a methodical approach we could eliminate 5-10 % of patients consulting for symptoms they attributed to EHS, but which actually did not prove to be related to EMFIS nor to EHS (see differential diagnosis).